Thursday, January 31, 2013
Look for the Union Label (ObamaTax Schadenfreude Part Deux)
Politically astute readers already know that The ObamaTax had major Union backing, both financially and manpower-wise. Now that it's in full-swing, though, those same folks are experiencing a bit of buyer's remorse:
"Union leaders say many of the law's requirements will drive up the costs for their health-care plans and make unionized workers less competitive"
Ya think?
They're counting on their lower-paid member having access to the much-touted "subsidies" that promise to lower their net cost. But as Bob pointed out earlier today, these subsidies are often elusive, meaning that the very folks that The ObamaTax was ostensibly designed to help may feel its pinch the worst.
So what's a Union to do?
Ah, so glad you asked:
"A handful of unions say they already have examined whether it makes sense to shift workers off their current plans and onto private coverage subsidized by the government."
Here's a free clue, fellas: Yes, yes it does.
But the winner of the coveted "Rocket Surgeon Union Honcho" has to be John Wilhelm, the leader of Unite Here Health, who:
"recalls standing next to Barack Obama at a rally in Nevada when he was a 2008 presidential candidate.
"I heard him say, 'If you like your health plan, you can keep it,' " Mr. Wilhelm recalled. Mr. Wilhelm said he expects the administration will craft a solution so that employer health-care plans won't be hurt. "If I'm wrong, and the president does not intend to keep his word, I would have severe second thoughts about the law."
Might want to clean those specs, Mr W.
"Union leaders say many of the law's requirements will drive up the costs for their health-care plans and make unionized workers less competitive"
Ya think?
They're counting on their lower-paid member having access to the much-touted "subsidies" that promise to lower their net cost. But as Bob pointed out earlier today, these subsidies are often elusive, meaning that the very folks that The ObamaTax was ostensibly designed to help may feel its pinch the worst.
So what's a Union to do?
Ah, so glad you asked:
"A handful of unions say they already have examined whether it makes sense to shift workers off their current plans and onto private coverage subsidized by the government."
Here's a free clue, fellas: Yes, yes it does.
But the winner of the coveted "Rocket Surgeon Union Honcho" has to be John Wilhelm, the leader of Unite Here Health, who:
"recalls standing next to Barack Obama at a rally in Nevada when he was a 2008 presidential candidate.
"I heard him say, 'If you like your health plan, you can keep it,' " Mr. Wilhelm recalled. Mr. Wilhelm said he expects the administration will craft a solution so that employer health-care plans won't be hurt. "If I'm wrong, and the president does not intend to keep his word, I would have severe second thoughts about the law."
Might want to clean those specs, Mr W.
Health Wonk Review - Waste, Warnings and the Future
Maggie Mahar hosts this week's roundup of wonky posts. Lots of material, well laid-out. Do stop by.
IRS to the Rescue

Employees can receive government tax credits to buy insurance for their families if the coverage their employers offer would cost more than 9.5 percent of their income, the IRS said today in final regulations. That calculation will be based on the cost of self-only coverage, not family coverage, which is more expensive and would give more people access to the credits.Bloomberg
So if you earn $50,000 (AGI) and you have a spouse and one child the government considers your employer based health insurance to be affordable as long as YOUR portion of the insurance does not exceed $4750 ($396 per month).
But if the cost to cover your family is another $1000 per month (definitely possible) your coverage is STILL affordable and "No subsidies for you!".
The IRS said in a proposed rule also issued today that most families in such a situation won’t have to pay a penalty to the government if they choose not to buy insurance.So, even though your coverage is not affordable you will not have to pay a penalty.
Suh-weet!
Truth AND Consequences

So, the ObamaTax Mandate is scheduled to take full effect in 11 short months.
Or is it?
"The Obama administration took new steps ... toward implementing the individual mandate ... downplaying the scope of the unpopular provision by stressing rules that allow exemptions from the requirement to purchase insurance."
Hmm, now where have we heard that before?
Oh yeah: ObamaWaiver Mania.
Aside from the fact that the mandate itself has no teeth (well, unless one is expecting a tax refund), what's the point?
Or, as HHS Secretary Shecantbeserious opines:
"The mandate penalty "applies only to the limited group of taxpayers who choose to spend a substantial period of time without coverage despite having ready access to affordable coverage"
Of course, since plans will be guaranteed issue, community rated and required to cover pre-existing conditions, wouldn't this apply to every policy? And if, according to their own calculations, fewer than 2% of us will have to pay any penalty, then what's the point?
And then there's this:
"Some families could get priced out of health insurance due to what's being called a [feature of the ObamaTax] ... families that can't afford the employer coverage that they are offered on the job will not be able to get financial assistance from the government to buy private health insurance on their own."
So they face a selectively enforced mandate that requires them to purchase insurance they can't afford but for which they're ineligible for subsidies. What could possibly go wrong?
Or is it?
"The Obama administration took new steps ... toward implementing the individual mandate ... downplaying the scope of the unpopular provision by stressing rules that allow exemptions from the requirement to purchase insurance."
Hmm, now where have we heard that before?
Oh yeah: ObamaWaiver Mania.
Aside from the fact that the mandate itself has no teeth (well, unless one is expecting a tax refund), what's the point?
Or, as HHS Secretary Shecantbeserious opines:
"The mandate penalty "applies only to the limited group of taxpayers who choose to spend a substantial period of time without coverage despite having ready access to affordable coverage"
Of course, since plans will be guaranteed issue, community rated and required to cover pre-existing conditions, wouldn't this apply to every policy? And if, according to their own calculations, fewer than 2% of us will have to pay any penalty, then what's the point?
And then there's this:
"Some families could get priced out of health insurance due to what's being called a [feature of the ObamaTax] ... families that can't afford the employer coverage that they are offered on the job will not be able to get financial assistance from the government to buy private health insurance on their own."
So they face a selectively enforced mandate that requires them to purchase insurance they can't afford but for which they're ineligible for subsidies. What could possibly go wrong?
Free money?

It's that time of year again: various tax services touting "maximum refund," sundry retailers with "suggestions" on how to spend those rebates, and the annual Flight of the W-2's as employers inform us how much we got paid last year.
Oh, and something new this year: Box 12.
"What the heck's a Box 12" you ask?
Thanks to The ObamaTax, it's how your employer informs you how much you paid for your health insurance last year.
"Now wait a gosh-darned minute there, Henry. I know how much I paid - I saw it coming out each week."
Um, no: that's how much you paid in addition to Box 12.
What, you thought your employer paid for any of your health insurance? Not paying attention, I see.
Bet you thought he paid those unemployment premiums and Social Security taxes, too. Now you know.
[Hat Tip: FoIB Holly R]
Oh, and something new this year: Box 12.
"What the heck's a Box 12" you ask?
Thanks to The ObamaTax, it's how your employer informs you how much you paid for your health insurance last year.
"Now wait a gosh-darned minute there, Henry. I know how much I paid - I saw it coming out each week."
Um, no: that's how much you paid in addition to Box 12.
What, you thought your employer paid for any of your health insurance? Not paying attention, I see.
Bet you thought he paid those unemployment premiums and Social Security taxes, too. Now you know.
[Hat Tip: FoIB Holly R]
Wednesday, January 30, 2013

Is there no virtue among us?
The difficult and heartbreaking public discussion continues over how to unravel the Newtown catastrophe and respond effectively. Everyone has ideas. Some of the ideas make sense to me, others do not, including the notion that increased regulation of mental health insurance benefits is a necessary part of the response.
More generally, politicians seem to think - and exhort the public to believe – that additional regulation or a new law is always the remedy for every problem. I think that mind-set needs examination.
Here’s an example of what I mean: In the Greater NY section of the WSJ this morning there’s an 18-paragraph article entitled “Conn. Ponders Mental Health.” [$link at this time] The article reports on progress of the state’s commission on mental health, appointed after Newtown. It observes that Connecticut “is moving toward sweeping changes” to its mental health laws including additional insurance mandates.
This movement is happening despite reported testimony of the chief psychiatrist at Hartford Hospital and a State Commission member, that because of privacy laws, it is impossible to ascertain whether the Newtown shooter was ever treated for mental illness and therefore “with nothing confirmed it is really impossible to say how changes in the mental health system could address his specific circumstances.”
As usual, telling information is buried at the end of the article. In the 16th paragraph we read: “Experts say the mental health parity laws [intended to force insurers to equalize benefits for mental health and physical health] aren’t adequately enforced.” In the 17th paragraph, an attorney notes that “we are supposed to have [mental health] parity, but it just doesn’t seem to play out in practice.” Is there any reason the public can expect that new laws or new regulations will be more strictly enforced? No. There is no reason.
Yet our politicians propose sweeping changes to mental health laws? Go figure.
In a better world, more of our so-called leaders would take the time to think rather than rush to enact even more laws that will be poorly-enforced and accomplish little (aside from attaching their names to bravely-titled, wordy, but ultimately worthless documents.)
So what’s to be done? I wish I knew. But I believe this is as true now as when it was first said more than 200 years ago:
“Is there no virtue among us? If there be not, we are in a wretched situation. No theoretical checks-no form of government can render us secure. To suppose that any form of government will secure liberty or happiness without any virtue in the people, is a chimerical idea”
--James Madison
More generally, politicians seem to think - and exhort the public to believe – that additional regulation or a new law is always the remedy for every problem. I think that mind-set needs examination.
Here’s an example of what I mean: In the Greater NY section of the WSJ this morning there’s an 18-paragraph article entitled “Conn. Ponders Mental Health.” [$link at this time] The article reports on progress of the state’s commission on mental health, appointed after Newtown. It observes that Connecticut “is moving toward sweeping changes” to its mental health laws including additional insurance mandates.
This movement is happening despite reported testimony of the chief psychiatrist at Hartford Hospital and a State Commission member, that because of privacy laws, it is impossible to ascertain whether the Newtown shooter was ever treated for mental illness and therefore “with nothing confirmed it is really impossible to say how changes in the mental health system could address his specific circumstances.”
As usual, telling information is buried at the end of the article. In the 16th paragraph we read: “Experts say the mental health parity laws [intended to force insurers to equalize benefits for mental health and physical health] aren’t adequately enforced.” In the 17th paragraph, an attorney notes that “we are supposed to have [mental health] parity, but it just doesn’t seem to play out in practice.” Is there any reason the public can expect that new laws or new regulations will be more strictly enforced? No. There is no reason.
Yet our politicians propose sweeping changes to mental health laws? Go figure.
In a better world, more of our so-called leaders would take the time to think rather than rush to enact even more laws that will be poorly-enforced and accomplish little (aside from attaching their names to bravely-titled, wordy, but ultimately worthless documents.)
So what’s to be done? I wish I knew. But I believe this is as true now as when it was first said more than 200 years ago:
“Is there no virtue among us? If there be not, we are in a wretched situation. No theoretical checks-no form of government can render us secure. To suppose that any form of government will secure liberty or happiness without any virtue in the people, is a chimerical idea”
--James Madison
Ch-ch-changes, HRA-style

The ObamaTax promises to touch just about anything and everything health insurance-related. A recent email informed us about the latest on The ObamaTax 's impact on Health Reimbursement Arrangements (HRAs):
"The preamble to [The ObamaTax] distinguished between HRAs that are "integrated" with a group health plan and HRAs that are "stand-alone." ... The question has been whether a stand-alone HRA can be quilted with individual health insurance coverage (not employer-sponsored group coverage) to satisfy the requirements."
I turned to our on-call Alternative Benefits Guru, Lou G, who explained that "there have been employers who would provide an HRA benefit to their employees who are not covered by the group health plan (they have individual coverage, or coverage through a spouse, no coverage at all etc). The IRS is saying that this is no longer allowed.
In order to have an HRA you must be enrolled in the group health plan, the concept of a "stand alone" HRA will not be permitted."
In other words, if you're not on the group plan, you don't get access to those sweet, sweet HRA dollars. But remember: if you like your health plan, you can keep your health plan.
[Hat Tip: Angela F and FoIB Jeff M]
"The preamble to [The ObamaTax] distinguished between HRAs that are "integrated" with a group health plan and HRAs that are "stand-alone." ... The question has been whether a stand-alone HRA can be quilted with individual health insurance coverage (not employer-sponsored group coverage) to satisfy the requirements."
I turned to our on-call Alternative Benefits Guru, Lou G, who explained that "there have been employers who would provide an HRA benefit to their employees who are not covered by the group health plan (they have individual coverage, or coverage through a spouse, no coverage at all etc). The IRS is saying that this is no longer allowed.
In order to have an HRA you must be enrolled in the group health plan, the concept of a "stand alone" HRA will not be permitted."
In other words, if you're not on the group plan, you don't get access to those sweet, sweet HRA dollars. But remember: if you like your health plan, you can keep your health plan.
[Hat Tip: Angela F and FoIB Jeff M]
MiniMed Maelstrom [UPDATED]

It had appeared that so-called MiniMed (aka "limited benefit") plans would be (for the most part) exempt from ObamaTax requirements. The ObamaTax itself seems to say that, but it's not really that simple (these things rarely are):
"[HHS Secretary Shecantbeserious] said the agency PPACA regulations include a number of rules governing when an indemnity policy included in an employer benefits package falls outside the PPACA framework."
The problem isn't necessarily with the plans themselves, but how they're integrated (or not) with employer-sponsored plans. There must be a fairly visible (if virtual) "wall of separation" between the traditional group plan and any MiniMeds that are purchased, and there have to be completely separate accounting and payroll deduction processes, which of course add to the employer's admin costs.
The plan must also be an indemnity-only configuration; that is, it "must pay a fixed dollar amount per day (or per other period) of hospitalization or illness (for example, $100 per day) regardless of the amount of expenses incurred." The problem comes from whether these benefits are calculated "per claim" or "per period." So, for example, if the plan reimburses $40 for a doctor's office visit, rather than $40 per day that you had medical services performed, there's a problem. Since this describes the bulk of plans that I've seen, this could be a big issue for employers that offer both "regular" and "limited benefit" type plans.
What's not clear to me right now (and I'll update this post as appropriate) is whether these rules apply to plans purchased by individual outside an employer rubric. If so, this could be a real problem for a lot of MiniMed marketers.
UPDATE: Perusing the linked FAQ, I see MiniMeds ("indemnity plans") referenced only in the context of an employer-sponsored plan:
"Fixed indemnity coverage under a group health plan meeting the conditions outlined in the Departments' regulations(3) is an excepted benefit"
and
"The Departments' regulations provide that a hospital indemnity or other fixed indemnity insurance policy under a group health plan provides excepted benefits" [emphasis added]
By the way, I think this:
"When a policy pays on a per-service basis as opposed to on a per-period basis, it is in practice a form of health coverage instead of an income replacement policy. Accordingly, it does not meet the conditions for excepted benefits."
is pure hokum. In a just world, Ms Shecantbeserious and her minions would find themselves in deep doo-doo for overstepping their regulatory bounds.
Fat chance of that, of course.
"[HHS Secretary Shecantbeserious] said the agency PPACA regulations include a number of rules governing when an indemnity policy included in an employer benefits package falls outside the PPACA framework."
The problem isn't necessarily with the plans themselves, but how they're integrated (or not) with employer-sponsored plans. There must be a fairly visible (if virtual) "wall of separation" between the traditional group plan and any MiniMeds that are purchased, and there have to be completely separate accounting and payroll deduction processes, which of course add to the employer's admin costs.
The plan must also be an indemnity-only configuration; that is, it "must pay a fixed dollar amount per day (or per other period) of hospitalization or illness (for example, $100 per day) regardless of the amount of expenses incurred." The problem comes from whether these benefits are calculated "per claim" or "per period." So, for example, if the plan reimburses $40 for a doctor's office visit, rather than $40 per day that you had medical services performed, there's a problem. Since this describes the bulk of plans that I've seen, this could be a big issue for employers that offer both "regular" and "limited benefit" type plans.
What's not clear to me right now (and I'll update this post as appropriate) is whether these rules apply to plans purchased by individual outside an employer rubric. If so, this could be a real problem for a lot of MiniMed marketers.
UPDATE: Perusing the linked FAQ, I see MiniMeds ("indemnity plans") referenced only in the context of an employer-sponsored plan:
"Fixed indemnity coverage under a group health plan meeting the conditions outlined in the Departments' regulations(3) is an excepted benefit"
and
"The Departments' regulations provide that a hospital indemnity or other fixed indemnity insurance policy under a group health plan provides excepted benefits" [emphasis added]
By the way, I think this:
"When a policy pays on a per-service basis as opposed to on a per-period basis, it is in practice a form of health coverage instead of an income replacement policy. Accordingly, it does not meet the conditions for excepted benefits."
is pure hokum. In a just world, Ms Shecantbeserious and her minions would find themselves in deep doo-doo for overstepping their regulatory bounds.
Fat chance of that, of course.
Tuesday, January 29, 2013
Pancreatic Cancer: Good News and Bad

It appears that a high-school student may have come up with an inexpensive, accurate and early method for detecting pancreatic cancer:
This is pretty important stuff: the disease kills over 95% of its victims, usually because it's difficult to detect in its early (more treatable) stages. Being able to catch it early on would be a real boon.
That's the good news.
The bad news, of course, is that The ObamaTax promises to severely limit additional research, let alone development of this new tech:
And since we're already seeing med-tech companies rapidly downsizing as a result of that tax, it's no sure thing that young Jack's new invention will ever see the light of day.
Too bad, that.
Shareholder Equity
Shareholder equity is a term very familiar to business owners and citizens that own stock. Quite simply, shareholder equity represents the net value of a company divided by the number of shareholders.
If you own stock in McDonalds (MCD) the shareholder equity is roughly $14 trillion which translates in to about $94 per share. McDonalds is a simple business based on delivering a consistent product to their customer base.
It is also a profitable business.
Profit is a dirty word to some but profit provides jobs and funds retirement for employees and . . . shareholders.
The United States also has shareholders in a manner of speaking. Just like McDonald's shareholders, U.S. citizens have a financial stake in the stability of the country.
The balance sheet of the U.S. doesn't look anything like the balance sheet of McDonalds. For the most part the U.S. government is devoid of any assets unless you want to count all those buildings and implements of destruction.
 But the U.S. does have debt.
But the U.S. does have debt.
Lot's of it.
About $16 trillion worth.
The shareholders, those responsible for funding the government, are now called taxpayers. You can't sell your share to anyone but you can pass it on to your children and grandchildren when you die. You can also pass it on to your spouse.
According to recent figures, if you are a taxpayer, your share of the federal debt is roughly $194,000 (CNS figures).
This does not include unfunded debt which is about 5x the accrued debt. But let's not worry about that for now.
What does all this have to do with health insurance?
More than you may think.
If all goes as planned, in January of 2014 citizens will be able to purchase health insurance through state and federal run exchanges. Many think this is a great thing for citizens and a windfall for health insurance carriers.
But if it is so great for the carriers, why are so many closing down their operations or indicating they will not participate in these exchanges? What could be better than a bunch of folks with money in hand (taxpayer subsidies) ready to buy health insurance? Even better, everyone is REQUIRED to have health insurance.
The folks in DC don't understand basic human psychology.
When something is free or heavily discounted it loses its' value and is subject to abuse. Consider free and government subsidized housing. How long do these places last before they are run down and in a state of disrepair?
Many doctors refuse to treat Medicaid patients. In part because of the low government reimbursement but also because of the attitude of many of their Medicaid patients.
Why is the government in the Medicaid business and not the insurance carriers?
Insurance carriers have shareholders who expect the carrier to participate in markets that are profitable. The government taxpayers (shareholders) really don't care if the government makes a profit or not and most of them don't know or comprehend the magnitude of their share of the national debt.
If you own a house and are still making mortgage payments you get a statement every year that shows how much you owe and how much you have paid on your loan during the prior year.
But the U.S. government doesn't do that. They don't send you a statement showing how much you have paid in taxes and how much you owe on the national debt.
Perhaps they should.
So why are carriers running away from the exchanges?
For the same reason they have no interest in sharing the risk of Medicaid patients. If health insurance carriers thought they could make a profit by offering insurance on the exchanges you would have to lock the door and beat them off with a stick.
But they are not clamoring to get in. They are running away. And the U.S. shareholders should be afraid.
Very afraid.
Because their share of the national debt is about to go up.
But of course they will never get a statement, so most will never know. But they will see their paychecks shrink.
And their shareholder equity rise . . . which is not a good thing.
If you own stock in McDonalds (MCD) the shareholder equity is roughly $14 trillion which translates in to about $94 per share. McDonalds is a simple business based on delivering a consistent product to their customer base.
It is also a profitable business.
Profit is a dirty word to some but profit provides jobs and funds retirement for employees and . . . shareholders.
The United States also has shareholders in a manner of speaking. Just like McDonald's shareholders, U.S. citizens have a financial stake in the stability of the country.
The balance sheet of the U.S. doesn't look anything like the balance sheet of McDonalds. For the most part the U.S. government is devoid of any assets unless you want to count all those buildings and implements of destruction.
Lot's of it.
About $16 trillion worth.
The shareholders, those responsible for funding the government, are now called taxpayers. You can't sell your share to anyone but you can pass it on to your children and grandchildren when you die. You can also pass it on to your spouse.
According to recent figures, if you are a taxpayer, your share of the federal debt is roughly $194,000 (CNS figures).
This does not include unfunded debt which is about 5x the accrued debt. But let's not worry about that for now.
What does all this have to do with health insurance?
More than you may think.
If all goes as planned, in January of 2014 citizens will be able to purchase health insurance through state and federal run exchanges. Many think this is a great thing for citizens and a windfall for health insurance carriers.
But if it is so great for the carriers, why are so many closing down their operations or indicating they will not participate in these exchanges? What could be better than a bunch of folks with money in hand (taxpayer subsidies) ready to buy health insurance? Even better, everyone is REQUIRED to have health insurance.
The folks in DC don't understand basic human psychology.
When something is free or heavily discounted it loses its' value and is subject to abuse. Consider free and government subsidized housing. How long do these places last before they are run down and in a state of disrepair?
Many doctors refuse to treat Medicaid patients. In part because of the low government reimbursement but also because of the attitude of many of their Medicaid patients.
Why is the government in the Medicaid business and not the insurance carriers?
Insurance carriers have shareholders who expect the carrier to participate in markets that are profitable. The government taxpayers (shareholders) really don't care if the government makes a profit or not and most of them don't know or comprehend the magnitude of their share of the national debt.
If you own a house and are still making mortgage payments you get a statement every year that shows how much you owe and how much you have paid on your loan during the prior year.
But the U.S. government doesn't do that. They don't send you a statement showing how much you have paid in taxes and how much you owe on the national debt.
Perhaps they should.
So why are carriers running away from the exchanges?
For the same reason they have no interest in sharing the risk of Medicaid patients. If health insurance carriers thought they could make a profit by offering insurance on the exchanges you would have to lock the door and beat them off with a stick.
But they are not clamoring to get in. They are running away. And the U.S. shareholders should be afraid.
Very afraid.
Because their share of the national debt is about to go up.
But of course they will never get a statement, so most will never know. But they will see their paychecks shrink.
And their shareholder equity rise . . . which is not a good thing.
Cannon Fire!
FoIB (and Cato Institute director of health policy studies) Michael Cannon fires another volley across the bow of ObamaTax advocates:
Monday, January 28, 2013
Unfortunate Agent Tricks - An Update

Oy, where to begin? One supposes that the beginning would be a good place:
"[Insurance agent] Mark String Sr pleaded not guilty to 59 counts of promotion of prostitution"
Generally speaking, this would not be auspicious. And, of course, it wasn't.
Now fast-forward a few months, and we learn about the latest "doings" in The Pine Tree State:
"The defense and the judge aren't happy with delays in the trial of the business partner in a prostitution scandal ... Prosecutors aren't happy, either, after the judge dismissed nearly four dozen charges."
And the jurors - sequestered for days on end - aren't exactly happy campers, either. Proceedings screeched to a halt late last week when Justice Nancy Mills "dismissed 46 of 59 counts" against Mr Strong. The latter, by the way, vehemently denies any untoward sexual contact between himself and Ms Zumba (or Zoomba - I've heard it both ways).
We'll continue to stay on top of the story as best we can.
"[Insurance agent] Mark String Sr pleaded not guilty to 59 counts of promotion of prostitution"
Generally speaking, this would not be auspicious. And, of course, it wasn't.
Now fast-forward a few months, and we learn about the latest "doings" in The Pine Tree State:
"The defense and the judge aren't happy with delays in the trial of the business partner in a prostitution scandal ... Prosecutors aren't happy, either, after the judge dismissed nearly four dozen charges."
And the jurors - sequestered for days on end - aren't exactly happy campers, either. Proceedings screeched to a halt late last week when Justice Nancy Mills "dismissed 46 of 59 counts" against Mr Strong. The latter, by the way, vehemently denies any untoward sexual contact between himself and Ms Zumba (or Zoomba - I've heard it both ways).
We'll continue to stay on top of the story as best we can.
Oh, Pew!
Bob noted this morning that folks who choose to engage in risky behavior (smoking, over-eating, etc) end up paying more for health insurance. But as (presumably responsible) adults are we doing enough to mitigate those very risks?
FoIB Holly R tips us to this Pew Research graphic, according to which we're making some strides:
FoIB Holly R tips us to this Pew Research graphic, according to which we're making some strides:
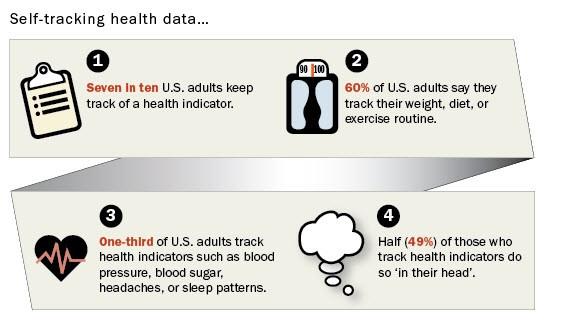
Frankly, though, I have to call BS on at least some of this. My guess is that what's really happening is that "60% of US adults CLAIM they track..."
And, of course, "tracking" doesn't necessarily lead to "doing something about it."
And, of course, "tracking" doesn't necessarily lead to "doing something about it."
Death Cab for Fatty

Annual health care costs are roughly $96 billion for smokers and $147 billion for the obese, the government says. These costs accompany sometimes heroic attempts to prolong lives, including surgery, chemotherapy and other measures.But despite these rescue attempts, smokers tend to die 10 years earlier on average, and the obese die five to 12 years prematurely, according to various researchers' estimates.
Deadbeats pay more when they borrow money. Careless and dangerous drivers pay more for health insurance.
Why shouldn't those with unhealthy lifestyles pay more for health insurance?
Smoking has the most obvious impact. Studies have increasingly shown harm to nonsmokers who are unlucky enough to work or live around heavy smokers. And several studies have shown heart attacks and asthma attack rates fell in counties or cities that adopted big smoking bans.The libertarian in me says we don't need more laws that impact personal freedom, but the capitalist side says that tobacco use is a choice and most obese people became overweight because of personal choice to overeat.
When you make a conscious choice to take on risky behavior you should expect to pay the price.
Friday, January 25, 2013

Another One (or Two) Bites the Dust
About those Obamacare health insurance exchanges . . .
As we get closer to the starting date it seems more carriers are getting cold feet, or at least indicating a very limited interest in playing the Obamacare game.
If this trend continues, and it will, no doubt the regime will blame the insurance carriers, Republicans and Bush.
As we get closer to the starting date it seems more carriers are getting cold feet, or at least indicating a very limited interest in playing the Obamacare game.
“Aetna has already declared that they do not believe their future is selling health insurance coverage in an environment where margins and profits are regulated by an 85% medical loss ratio. They believe their revenues and earnings growth will be from the sale of their intellectual and system assets to the ACOs and exchanges and from offshore opportunities. Cigna has expressed similar strategies.”AIS
If this trend continues, and it will, no doubt the regime will blame the insurance carriers, Republicans and Bush.
A very expensive butt
No, not that kind; this kind:
"Millions of smokers could be priced out of health insurance because of tobacco penalties in [The ObamaTax] ... allows health insurers to charge smokers buying individual policies up to 50 percent higher premiums"
This is hysterically funny.
First, since health insurance plans will be guaranteed issue, pre-existing conditions covered almost immediately, and insurers are essentially prohibited from cancelling for anything short of failing to pay the premium, what possible penalty could there be for lying on the enrollment form?
[Since plans are guaranteed issue, they're not applications]
But wait, it gets better:
"[G]overnment tax credits that will be available to help pay premiums cannot be used to offset the cost of penalties for smokers."
So again, why would anyone disclose tobacco use?
But wait, it gets even better:
"For a 55-year-old smoker, the penalty could reach nearly $4,250 a year."
That's in addition to the underlying premium, which is already inflated due to - you guessed it - guaranteed issue and community rating requirements. A very realistic annual premium, then, would be north of $10,000. But thepenalty tax for going bare is a fraction of that. So again, why would this poor smoker even bother to purchase insurance until the very last minute?
The mind boggles.
"Millions of smokers could be priced out of health insurance because of tobacco penalties in [The ObamaTax] ... allows health insurers to charge smokers buying individual policies up to 50 percent higher premiums"
This is hysterically funny.
First, since health insurance plans will be guaranteed issue, pre-existing conditions covered almost immediately, and insurers are essentially prohibited from cancelling for anything short of failing to pay the premium, what possible penalty could there be for lying on the enrollment form?
[Since plans are guaranteed issue, they're not applications]
But wait, it gets better:
"[G]overnment tax credits that will be available to help pay premiums cannot be used to offset the cost of penalties for smokers."
So again, why would anyone disclose tobacco use?
But wait, it gets even better:
"For a 55-year-old smoker, the penalty could reach nearly $4,250 a year."
That's in addition to the underlying premium, which is already inflated due to - you guessed it - guaranteed issue and community rating requirements. A very realistic annual premium, then, would be north of $10,000. But the
The mind boggles.
Thursday, January 24, 2013
Cute, but naive: LTCi and DNA

Long Term Care insurance is one of the two most complicated products we sell. There are a lot of "moving parts," and underwriting is especially important. These plans represent a tremendous risk for carriers (and are priced to reflect this, of course). One factor upon which they rely is ones' family history and, sometimes, one's actual genetic predisposition.
As we've discussed previously, the use of genetic information in insurance underwriting is - to put it mildly - controversial. Under the Genetic Information Nondiscrimination Act (which dates back to 2008), health insurance carriers are proscribed from its use. But LTCi has not been considered "health insurance" and so was exempt from this prohibition.
Now, HHS Secretary Shecantbeserious is weighing the possibility of unilaterally changing that.
In a post at LifeHealthPro, actuary and LTCi wholesaler Claude Thau makes the case against her doing so, but undermines himself from almost the very start:
"A belief on the part of HHS that it has the right to unilaterally expand GINA would be similar to HHS’s position on the CLASS Act ... The separation of powers is the genius of the U.S. Constitution and it would be scary to me to see the Executive Branch undermine the constitution in that regard"
Cue laughtrack.
Since when has Madame Kathy cared a whit about overstepping her authority? Perhaps Mr Thau should consult with the owners of Domino's and Hobby Lobby about "unilateral expansion." Heck, she even offers advice on how insureds should defraud their carriers. Does he really think there are depths to which she wouldn't willingly plunge?
I sure don't.
As we've discussed previously, the use of genetic information in insurance underwriting is - to put it mildly - controversial. Under the Genetic Information Nondiscrimination Act (which dates back to 2008), health insurance carriers are proscribed from its use. But LTCi has not been considered "health insurance" and so was exempt from this prohibition.
Now, HHS Secretary Shecantbeserious is weighing the possibility of unilaterally changing that.
In a post at LifeHealthPro, actuary and LTCi wholesaler Claude Thau makes the case against her doing so, but undermines himself from almost the very start:
"A belief on the part of HHS that it has the right to unilaterally expand GINA would be similar to HHS’s position on the CLASS Act ... The separation of powers is the genius of the U.S. Constitution and it would be scary to me to see the Executive Branch undermine the constitution in that regard"
Cue laughtrack.
Since when has Madame Kathy cared a whit about overstepping her authority? Perhaps Mr Thau should consult with the owners of Domino's and Hobby Lobby about "unilateral expansion." Heck, she even offers advice on how insureds should defraud their carriers. Does he really think there are depths to which she wouldn't willingly plunge?
I sure don't.
Wednesday, January 23, 2013
Playing Chicken
You may remember the game of "chicken" from your youth. Usually a lot of testosterone in the air as two males seek to prove which one is better in hopes of winning the affection of a female.
In case you forgot, perhaps this scene from the original Footloose will refresh your memory. Kevin Bacon and some other guy are trying to win the heart of the hot girl played by Lori Singer. Instead of cars, they used tractors.
Seems we have an updated version of chicken, but this time it is health insurance companies vs. the Obamacare exchanges. It doesn't appear the carriers are embracing this idea with open arms.
First out was insurance behemoth UHC saying "Maybe Not".
Now the folks at Wellpoint are on the dance floor and making similar comments.
So will Wellpoint go all in, or will they play chicken when it comes to the exchanges?
Guess we will have to wait and see.
Did I mention Lori Singer is hot?
Thanks to Henry Stern for this tip.
In case you forgot, perhaps this scene from the original Footloose will refresh your memory. Kevin Bacon and some other guy are trying to win the heart of the hot girl played by Lori Singer. Instead of cars, they used tractors.
Seems we have an updated version of chicken, but this time it is health insurance companies vs. the Obamacare exchanges. It doesn't appear the carriers are embracing this idea with open arms.
First out was insurance behemoth UHC saying "Maybe Not".
Now the folks at Wellpoint are on the dance floor and making similar comments.
Wayne Deveydt, WellPoint's chief financial officer, said the company believes it is entering 2013 on a strong note.Life Health Pro
But uncertainty federal budget actions, overall medical utilization trends, the severity of the 2012-2013 flu season, and implementation of the Patient Protection and Affordable Care Act of 2010 (PPACA) are good reasons for WellPoint to be cautious when predicting what might happen to earnings this year, Deveydt said.
So will Wellpoint go all in, or will they play chicken when it comes to the exchanges?
Guess we will have to wait and see.
Did I mention Lori Singer is hot?
Thanks to Henry Stern for this tip.
Network Numbness

From email I received this morning:
"Kettering Anesthesia Associates, which serves [various providers in the Dayton, OH area], has chosen to terminate its provider contract with Anthem ... Consequently, Anthem members may be billed by Kettering Anesthesia Associates for any balance not covered by Anthem"
This is SOP when dealing with network-based plans: with some exceptions, providers are barred from "balance billing" their patients for amounts written off as discounts. The big problem here is that PARE providers generally have an exclusive relationship with hospitals; that is, if you're going to be "put under" at (for example) Kettering Hospital, you don't have a choice of gas-passers. If they're not in-network, they can bill you pretty much anything they want, and you're on the hook.
[As an aside, I was quite surprised to learn that KAA was even in a network: that's highly unusual]
On the plus side, I must commend Anthem for recognizing this:
"[S]ince our members do not have a choice of anesthesiologists for surgeries performed at Kettering Medical Center, Anthem will apply the equivalent of any member liability amounts such as co-payments, deductibles, etc., at the member’s in-network level (rather than the out-of-network benefit level equivalent). In most circumstances, payment for services will be issued to the member"
Two things of interest here: first, that they'll essentially continue to treat these claims as in-network, so as not to penalize their members. Second, I love that they're going to send that balance due amount directly to the insured. This accomplishes several things: it increases patients' awareness of just how much their health care costs, and it also puts the onus on the provider to collect whatever's due (something we mentioned almost 7 years ago).
Kudos to Anthem on a clever and effective solution to what could have been a major snafu.
[Hat Tip: Beth D]
"Kettering Anesthesia Associates, which serves [various providers in the Dayton, OH area], has chosen to terminate its provider contract with Anthem ... Consequently, Anthem members may be billed by Kettering Anesthesia Associates for any balance not covered by Anthem"
This is SOP when dealing with network-based plans: with some exceptions, providers are barred from "balance billing" their patients for amounts written off as discounts. The big problem here is that PARE providers generally have an exclusive relationship with hospitals; that is, if you're going to be "put under" at (for example) Kettering Hospital, you don't have a choice of gas-passers. If they're not in-network, they can bill you pretty much anything they want, and you're on the hook.
[As an aside, I was quite surprised to learn that KAA was even in a network: that's highly unusual]
On the plus side, I must commend Anthem for recognizing this:
"[S]ince our members do not have a choice of anesthesiologists for surgeries performed at Kettering Medical Center, Anthem will apply the equivalent of any member liability amounts such as co-payments, deductibles, etc., at the member’s in-network level (rather than the out-of-network benefit level equivalent). In most circumstances, payment for services will be issued to the member"
Two things of interest here: first, that they'll essentially continue to treat these claims as in-network, so as not to penalize their members. Second, I love that they're going to send that balance due amount directly to the insured. This accomplishes several things: it increases patients' awareness of just how much their health care costs, and it also puts the onus on the provider to collect whatever's due (something we mentioned almost 7 years ago).
Kudos to Anthem on a clever and effective solution to what could have been a major snafu.
[Hat Tip: Beth D]
Health insurance? Aisle 12

[Oy - scooped AGAIN! Still, mine is a bit different take on the subject. HGS]
This may start in the Golden State, but don't doubt for a New York minute that it won't catch on across the country:
"The California Health Benefit Exchange board is hoping to get retail stores to provide in-store enrollment assistance for the state's [ObamaExchange] ... Members of the ... team believe that retail stores are good vehicles for reaching uninsured residents"
In theory, these "trained and certified" employees would be able to help you choose a melon and a health plan. I have my doubts: one doesn't see a lot of rocket surgeons wearing those bright blue or red, pin-emblazoned vests. On the other hand, given how The ObamaTax policies must be structured, it wouldn't take a rocket surgeon to explain them, either.
Perhaps the model isn't the guy stocking the shelves, but the butcher or pharmacist behind a counter. That seems to me a bit more workable: someone tasked with handling the insurance questions, not where one can find the canned soups.
And I can't help but think that this is doomed to failure: after all, how would the store make money on this deal? They can "provide Tier 2 marketing support, by helping with marketing, education and referral activities, but not with actual enrollment services," but why would they? After all, they're taking all the risk (what if their advice is bad and they're sued or fined?) for zero financial reward.
Of course real, professional agents won't be much better off if they agree to become ObamaExchange Navigators, since "they cannot get compensation from the insurers selling products through a state's PPACA exchange program."
I know - we'll make up for it in volume!
This may start in the Golden State, but don't doubt for a New York minute that it won't catch on across the country:
"The California Health Benefit Exchange board is hoping to get retail stores to provide in-store enrollment assistance for the state's [ObamaExchange] ... Members of the ... team believe that retail stores are good vehicles for reaching uninsured residents"
In theory, these "trained and certified" employees would be able to help you choose a melon and a health plan. I have my doubts: one doesn't see a lot of rocket surgeons wearing those bright blue or red, pin-emblazoned vests. On the other hand, given how The ObamaTax policies must be structured, it wouldn't take a rocket surgeon to explain them, either.
Perhaps the model isn't the guy stocking the shelves, but the butcher or pharmacist behind a counter. That seems to me a bit more workable: someone tasked with handling the insurance questions, not where one can find the canned soups.
And I can't help but think that this is doomed to failure: after all, how would the store make money on this deal? They can "provide Tier 2 marketing support, by helping with marketing, education and referral activities, but not with actual enrollment services," but why would they? After all, they're taking all the risk (what if their advice is bad and they're sued or fined?) for zero financial reward.
Of course real, professional agents won't be much better off if they agree to become ObamaExchange Navigators, since "they cannot get compensation from the insurers selling products through a state's PPACA exchange program."
I know - we'll make up for it in volume!
Walmartian Insurance

To participate in "Tier 1 retail partnerships" with the Covered California exchange, a store would have to get employees trained and certified as providers of in-person assistance, according to a written presentation prepared by Thien Lam, a deputy director at the boardLife Health Pro
Trained and certified. Doesn't say licensed as is the case for insurance agents.
Stores not willing or able to get employees certified as in-person assisters could provide Tier 2 marketing support, by helping with marketing, education and referral activities, but not with actual enrollment services, and other stores could provide Tier 3 support, by putting up posters, distributing flyers and adding messages about Covered California to store bags and cash register receipts, Lam said.
Posters and flyers. Surprised they didn't think of having folks dressed up like Uncle Sam or HHS Sebelius waving signs on street corners.
Now isn't that special?
Hurry Up and Die

The government confirms this by stating "the elderly are an unnecessary drain on the country's finances".
Taro Aso said, "the elderly should be allowed to "hurry up and die" to relieve pressure on the state to pay for their medical care."
If the name Taro Aso doesn't ring a bell, there is probably a reason why. Mr. Aso is the Finance Minister for Japan.
"I see people aged 67 or 68 at class reunions who dodder around and are constantly going to the doctor," he said at a meeting of economists. "Why should I have to pay for people who just eat and drink and make no effort? I walk every day and do other things, but I'm paying more in taxes."
"Heaven forbid if you are forced to live on when you want to die. I would wake up feeling increasingly bad knowing that [treatment] was all being paid for by the government," he said during a meeting of the national council on social security reforms. "The problem won't be solved unless you let them hurry up and die."UK Guardian
But wait. This isn't just about old people on Medicare. In Japan EVERYONE is on taxpayer funded health care.
Aso's comments are likely to cause offence in Japan, where almost a quarter of the 128 million population is aged over 60. The proportion is forecast to rise to 40% over the next 50 years.
Japan's population composition and projections are similar to what we have in the U.S.
Wonder how folks on U.S. Medicare feel about this?
Not your problem you say? That is Japan, not the U.S. and you are not on Medicare.
You are not on Medicare . . . yet.
John Kerry on How to Kill Medicare
Medicare has always been a failure measured by what it was supposed to accomplish: protect Grandma from losing the shirt off her back, and cost. But it was a very popular failure. Conservatives have wondered for years how to rid the nation of this albatross. Thankfully John Kerry has struck the first blow for freedom:
"Meanwhile, John Kerry found another way to raid the health care system. The Senator from Massachusetts did what diligent Senators do; he added a provision to the Affordable Care Act to allow his state’s hospitals to increase their Medicare reimbursements by a factor of ten:
MA is a small State, it took some chutzpah to pull this off. Other states and hospitals are obviously not going to stand for this. Luckily for the taxpayers we are broke, so they can't just give every hospital a 10-fold pay raise. The more states fight over the small pot of blood money and more games like this the politicians play the sooner the public will see this for the failure it is and get rid of it.
"Meanwhile, John Kerry found another way to raid the health care system. The Senator from Massachusetts did what diligent Senators do; he added a provision to the Affordable Care Act to allow his state’s hospitals to increase their Medicare reimbursements by a factor of ten:
Here’s how Massachusetts gets extra money: Hospitals in urban areas have to be paid at least the same amount as rural hospitals. Massachusetts only has one rural hospital—a 19-bed facility on Nantucket island. So, the Nantucket Cottage Hospital sets the floor for every hospital in the state.If the provision remains in place, Massachusetts’s payments will rise over the next decade from $367 million to about $3.5 billion. The pool operates on a zero-sum basis, so all the money the Bay State gets will be funded by cutbacks from other states."
But because Nantucket is so wealthy, its cost of living is high—and thus so are its Medicare payments. That drives up the payments for every other hospital in the state. And under Kerry’s provision in the Affordable Care Act, hospital payments come from a nationwide pool.
MA is a small State, it took some chutzpah to pull this off. Other states and hospitals are obviously not going to stand for this. Luckily for the taxpayers we are broke, so they can't just give every hospital a 10-fold pay raise. The more states fight over the small pot of blood money and more games like this the politicians play the sooner the public will see this for the failure it is and get rid of it.
Well Duh! then how much higher?
Bob discussed a WSJ blog explaining why rates are going to go up. Forbes has a hint just how bad it might be and early discussion of pushing back some of the expensive parts:
"A California insurance broker, who sells health plans to individuals and small businesses, told me that she’s prepping her clients for a sticker shock. Her local carriers are hinting to her that premiums may triple this fall, when the plans unveil how they’ll billet the full brunt of Obamacare’s new regulations and mandates."
"There’s buzz in Washington that to ease the price hikes, the Obama team may slow down some of the most expensive regulations. This might include the law’s mandatory community rating. One approach they’re said to be considering is allowing some of the historically based underwriting to stay in place for a time."
Obama already started most of the taxes after his reelection; who would be surprised that in order to protect his legacy he pushes the worst parts of ACA onto the next President? Let them figure out how to fulfill his promises or take the blame for repealing Obamacare, all he cares about is getting credit for covering 30 million people and fixing healthcare. Neither of those things have to actually happen: the MSM has already credited him with accomplishing these goals
It will be amusing to watch Obama and the Media dance their way out of this way. Plenty more to come.
"A California insurance broker, who sells health plans to individuals and small businesses, told me that she’s prepping her clients for a sticker shock. Her local carriers are hinting to her that premiums may triple this fall, when the plans unveil how they’ll billet the full brunt of Obamacare’s new regulations and mandates."
"There’s buzz in Washington that to ease the price hikes, the Obama team may slow down some of the most expensive regulations. This might include the law’s mandatory community rating. One approach they’re said to be considering is allowing some of the historically based underwriting to stay in place for a time."
Obama already started most of the taxes after his reelection; who would be surprised that in order to protect his legacy he pushes the worst parts of ACA onto the next President? Let them figure out how to fulfill his promises or take the blame for repealing Obamacare, all he cares about is getting credit for covering 30 million people and fixing healthcare. Neither of those things have to actually happen: the MSM has already credited him with accomplishing these goals
It will be amusing to watch Obama and the Media dance their way out of this way. Plenty more to come.
Well Duh!

Central to ObamaCare are requirements that health insurers (1) accept everyone who applies (guaranteed issue), (2) cannot charge more based on serious medical conditions (modified community rating), and (3) include numerous coverage mandates that force insurance to pay for many often uncovered medical conditions.
Guaranteed issue incentivizes people to forgo buying a policy until they get sick and need coverage (and then drop the policy after they get well).
Which leads to a "startling revelation".
How do we know these requirements will have such a negative impact on premiums? Eight states—New Jersey, New York, Maine, New Hampshire, Washington, Kentucky, Vermont and Massachusetts—enacted guaranteed issue and community rating in the mid-1990s and wrecked their individual (i.e., non-group) health-insurance markets. Premiums increased so much that Kentucky largely repealed its law in 2000 and some of the other states eventually modified their community-rating provisions.
Yes, higher rates are coming.
A LOT higher.
Deal with it.
Cavalcade of Risk #175: A Lighter Side of Risk
Julie Ferguson hosts a light-hearted edition of our bi-weekly collection of risky posts. There's little risk that you won't be amused and enlightened.
So drop by for a laugh, and stay for an insight (or three).
So drop by for a laugh, and stay for an insight (or three).
Tuesday, January 22, 2013
Schooling the ObamaTax

As we reported in November, higher education employment opportunities are on the chopping block thanks to the ObamaTax. In just a few short months, the ripple effect has continued to grow:
"A handful of schools, including Community College of Allegheny County in Pennsylvania and Youngstown State University in Ohio, have curbed the number of classes that adjuncts can teach in the current spring semester to limit the schools' exposure to the health-insurance requirement."
Interesting choice of words: "handful." Kinda minimizes the problem, doesn't it? Well maybe for the "ins," but not so much for folks like instructor Robert Balla, who "faces a new cap on the number of hours he can teach at Stark State College. In a Dec. 6 letter, the North Canton school told him that "in order to avoid penalties under the Affordable Care Act…employees with part-time or adjunct status will not be assigned more than an average of 29 hours per week."
Mr Balla, it should be noted, teaches (among other things) technical writing, and is well thought-of by his students. But that doesn't matter under the ObamaTax, and now his students (and prospective students) are worse off for it.
On the other hand, he's apparently bought into the popular (yet erroneous) assumption that the ObamaTax would result in lower costs and better coverage:
"In education, we're working for the public good, we are public employees at a public institution; we should be the first ones to uphold the law, to set the example."
No, you're providing a service for a fee, much like health care providers. Perhaps we need to mandate a college education, as well. What could possibly go wrong?
[Hat Tip: FoIB Holly R]
"A handful of schools, including Community College of Allegheny County in Pennsylvania and Youngstown State University in Ohio, have curbed the number of classes that adjuncts can teach in the current spring semester to limit the schools' exposure to the health-insurance requirement."
Interesting choice of words: "handful." Kinda minimizes the problem, doesn't it? Well maybe for the "ins," but not so much for folks like instructor Robert Balla, who "faces a new cap on the number of hours he can teach at Stark State College. In a Dec. 6 letter, the North Canton school told him that "in order to avoid penalties under the Affordable Care Act…employees with part-time or adjunct status will not be assigned more than an average of 29 hours per week."
Mr Balla, it should be noted, teaches (among other things) technical writing, and is well thought-of by his students. But that doesn't matter under the ObamaTax, and now his students (and prospective students) are worse off for it.
On the other hand, he's apparently bought into the popular (yet erroneous) assumption that the ObamaTax would result in lower costs and better coverage:
"In education, we're working for the public good, we are public employees at a public institution; we should be the first ones to uphold the law, to set the example."
No, you're providing a service for a fee, much like health care providers. Perhaps we need to mandate a college education, as well. What could possibly go wrong?
[Hat Tip: FoIB Holly R]
Subscribe to:
Comments (Atom)